
One of the most common shoulder injuries, acromioclavicular joint (ACJ) dislocations account for around 9% of shoulder girdle injuries
 Usual cause is a direct blow to the superior aspect of the shoulder forcing the scapula down and leading to damage to to the AC and coracoclavicular (CC) ligaments – see diagram.
Usual cause is a direct blow to the superior aspect of the shoulder forcing the scapula down and leading to damage to to the AC and coracoclavicular (CC) ligaments – see diagram.
This is injury is more common in
- males
- athletes (especially full contact)
- ages between around 20-40
It is classified Grade I-VI (Rockwood classification) with I representing a sprain with no radiographical signs and V&VI significant displacement of the clavicle.
Examination
- The patient will express pain at the ACJ and have tenderness over this point.
- Cross arm adduction will illicit pain at the ACJ (a blunt test for problems with ACJ – maybe chronic or acute)
- Altered contour of the shoulder at the ACJ compared to other side.
Diagnosis and classification is made clinically and radiographically
Normal and Grade I

There is a gap visible between the distal clavicle and acromion (5-8 mm – narrower in the elderly)
There may be a small amount of widening of the joint space in Grade I
The inferior borders should align.
Grade II

There is widening of the ACJ space
The inferior border of the clavicle is raised in respect to the acromion but not above its superior border.
Note the altered soft tissue line over the superior edge of the distal clavicle.
Grade III
The inferior border of the clavicle is raised in respect to the acromion above its superior border.
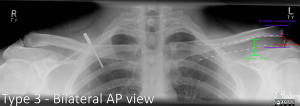
Grade IV
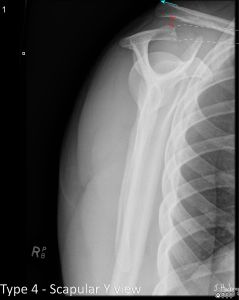
The clavicle is displaced posterior into the trapezius.
Grade V
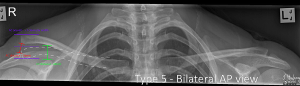
The Clavicle is markedly elevated with coracoclavicular distance more than twice normal.
Grade VI
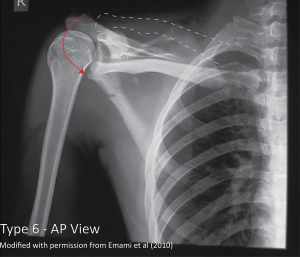
The clavicle is inferiorly displaced behind coracobrachialis and biceps tendons.
Comparative views can be useful if you are clinically suspicious of an ACJ injury, but normal AP views are not conclusive.
Treatment and Referral
All Grades
Manage in a sling
refer to Upper Limb Physio.
Grade I&II likely managed conservatively.
Grade III management varies dependant on specialist and patient.
Grade IV-VI likely to need surgery (though recent studies suggest no difference in functional outcomes between operative and nonoperative interventions for high grade injuries. OrthoBullets, 2025)
Further reading
With thanks to
www.shoulderdoc.co.uk/article/60
www.orthobullets.com/shoulder-and-elbow/3047/acromio-clavicular-injuries-ac-separation
radiopaedia.org/articles/acromioclavicular-injury?lang=gb
radiopaedia.org/cases/rockwood-classification-of-acromioclavicular-joint-injury-annotated-radiographs-1?lang=us