High Consequence Infectious Diseases (HCIDs) include a group of rare but severe infections that require
ACTIONS – CARD HERE
- Immediate isolation
- Enhanced PPE
- Early specialist involvement.
High Consequence Infectious Diseases (HCIDs) include a group of rare but severe infections that require
Recent Incident: Bat contact was not recognised (effectively touching a bat without gloves means treatment is recommended)
Important: Rabies Vaccine is in short supply and we must do a UKHSA risk assessment. Call RIgS 09:30-17:00 7 days, OR complete Form

Rabies is an acute viral encephalomyelitis caused by members of the lyssavirus genus. The UK has been declared “Rabies-Free”. However, it is known that even in “Rabies-Free” counties the bat population posse a risk.
In the UK the only bat to carry rabies is the Daubenton’s Bat [Picture on the Left] and this is not a common bat in the UK. The UK and Ireland are Classified as “low-risk” for bat exposure. Despite our “low-risk” status in 2002 a man died from rabies caught in the UK from bat exposure.
Although rabies is rare it is fatal so we must treat appropriately, Public Health England – Green book details this.
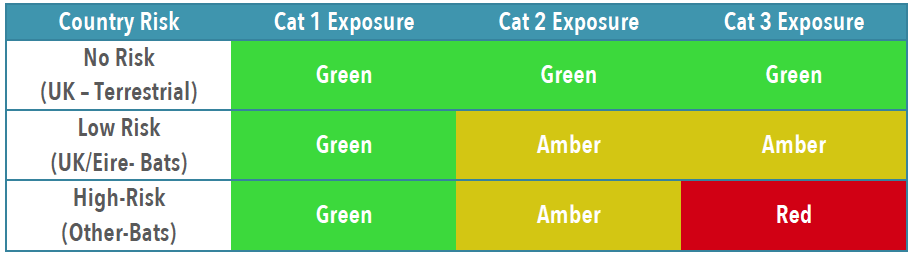
To establish patients risk and thus treatment you need to establish the Exposure Category and Country Risk [Link to Country Risk]

Obviously patients with wounds will need appropriate wound care and cleaning, specifics for rabies are below.
If in ANY doubt, or you feel you need advice about treatment contact: On-Call Microbiologist (who will contact PHE or Virology advice)

You will likely need to liaise with the duty pharmacist to obtain vaccine or HRIG – which may need to be sent from a different hospital. [it is probably worth trying to obtain the 1st weeks treatment if possible, to avoid treatment delays]
IN HOURS 08:30AM-5PM PLEASE CALL PHARMACY TO INFORM THEM TO EXPECT A DELIVERY OF IMMUNOGLOBULIN SO THIS CAN BE SEGREGATED FOR THE CORRECT PATIENT. PLEASE ASK TO SPEAK TO THE RESPONSIBLE PHARMACIST CRH (4218/4279) HRI (2422/7123)
Rabies and Immunoglobulin Service (RIgS), National Infection Service, Public Health England, Colindale (PHE Colindale Duty Doctor out of hours): 0208 327 6204 or 0208 200 4400
Prevent the spread of infections by ensuring: routine immunisation, high standards of personal hygiene and practice, particularly hand-washing, and maintaining a clean environment. However, the Health Protection Agency recommend exclusion in some conditions. The table below is up to date as of December 2025 but ideally check the HPA website directly.
The prevalence of Tuberculosis in our region is increasing and has significant issues for both the patient and public health if we miss it.

try the Emergency Drug Cupboard

There have been >100 patients identified as having Mpox in the UK during the current outbreak. Most of these cases have been amongst men who have sex with men.
Reports have suggested that although lesions occur any where including palms and soles. Genital lessons and lymphadenopathy are very common
March 2024 – UKHSA warn there is increasing cases in DRC (Democratic Republic of Congo), so stay vigilant in travellers from central Africa.
Study Running – Send Urine Sample prior to Antibiotics
(if this does not interfere with treatment of Red-Flag Sepsis)
Imaging in ED is only required if ED suspects: