High Consequence Infectious Diseases (HCIDs) include a group of rare but severe infections that require
ACTIONS – CARD HERE
- Immediate isolation
- Enhanced PPE
- Early specialist involvement.
High Consequence Infectious Diseases (HCIDs) include a group of rare but severe infections that require

Severe pain is the most common reason that patients with sickle cell, will attend the ED. The pain can be agonising (and often underestimated by us), we need to act fast to help ease the symptoms
Read more
Aortic Dissection (AD), is uncommon (1 AD:200 ACS) but is…Rapidly FATAL! Unfortunately recognising aortic dissection is difficult with a clinician pickup rate of 15-43%. Read more
Recent Incident: Bat contact was not recognised (effectively touching a bat without gloves means treatment is recommended)
Important: Rabies Vaccine is in short supply and we must do a UKHSA risk assessment. Call RIgS 09:30-17:00 7 days, OR complete Form

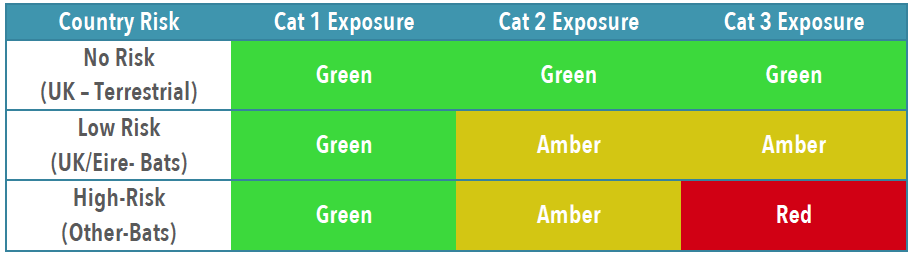
Rabies is an acute viral encephalomyelitis caused by members of the lyssavirus genus. The UK has been declared “Rabies-Free”. However, it is known that even in “Rabies-Free” counties the bat population posse a risk.
In the UK the only bat to carry rabies is the Daubenton’s Bat [Picture on the Left] and this is not a common bat in the UK. The UK and Ireland are Classified as “low-risk” for bat exposure. Despite our “low-risk” status in 2002 a man died from rabies caught in the UK from bat exposure.
Although rabies is rare it is fatal so we must treat appropriately, Public Health England – Green book details this.
To establish patients risk and thus treatment you need to establish the Exposure Category and Country Risk [Link to Country Risk]

Obviously patients with wounds will need appropriate wound care and cleaning, specifics for rabies are below.
If in ANY doubt, or you feel you need advice about treatment contact: On-Call Microbiologist (who will contact PHE or Virology advice)

You will likely need to liaise with the duty pharmacist to obtain vaccine or HRIG – which may need to be sent from a different hospital. [it is probably worth trying to obtain the 1st weeks treatment if possible, to avoid treatment delays]
IN HOURS 08:30AM-5PM PLEASE CALL PHARMACY TO INFORM THEM TO EXPECT A DELIVERY OF IMMUNOGLOBULIN SO THIS CAN BE SEGREGATED FOR THE CORRECT PATIENT. PLEASE ASK TO SPEAK TO THE RESPONSIBLE PHARMACIST CRH (4218/4279) HRI (2422/7123)
Rabies and Immunoglobulin Service (RIgS), National Infection Service, Public Health England, Colindale (PHE Colindale Duty Doctor out of hours): 0208 327 6204 or 0208 200 4400
This is guide to the investigation of Metastatic Spinal Cord Compression (MSCC) in Oncology/Haematology patients. – (Trust link)
You need to be a bit more suspicious and have a lower threshold for investigation than in patients without Known, Suspected OR Previous Malignancy Read more
Eating disorders* are relatively common and unfortunately patients who “look well” can have a significant mortality risk. MEED.org.uk have national risk tools to recognise those that would benefit from admission, which fit with our local mental health teams, and agreed by both acute medicine and paediatrics
(*anorexia nervosa, bulimia nervosa, binge eating or avoidant restrictive food intake disorder)
Anyone with one or more RED’s is high risk and should be considered for admission MEED
If anybody is symptomatic after button battery ingestion they need referral to the Surgical team for urgent endoscopic removal. Liase immediately with our local surgical/ENT teams but be aware this may end up as a time critical transfer to Leeds especially if child <2years. Read more
Mind the Gap is a handbook of clinical signs in black and brown skins
Another excellent resource, especially for childhood rashes is the website SKINDEEP.
![]()

