
Aortic Dissection (AD), is uncommon (1 AD:200 ACS) but is…Rapidly FATAL! Unfortunately recognising aortic dissection is difficult with a clinician pickup rate of 15-43%. Read more
Aortic Dissection (AD), is uncommon (1 AD:200 ACS) but is…Rapidly FATAL! Unfortunately recognising aortic dissection is difficult with a clinician pickup rate of 15-43%. Read more
Recent Incident: Bat contact was not recognised (effectively touching a bat without gloves means treatment is recommended)
Important: Rabies Vaccine is in short supply and we must do a UKHSA risk assessment. Call RIgS 09:30-17:00 7 days, OR complete Form

Rabies is an acute viral encephalomyelitis caused by members of the lyssavirus genus. The UK has been declared “Rabies-Free”. However, it is known that even in “Rabies-Free” counties the bat population posse a risk.
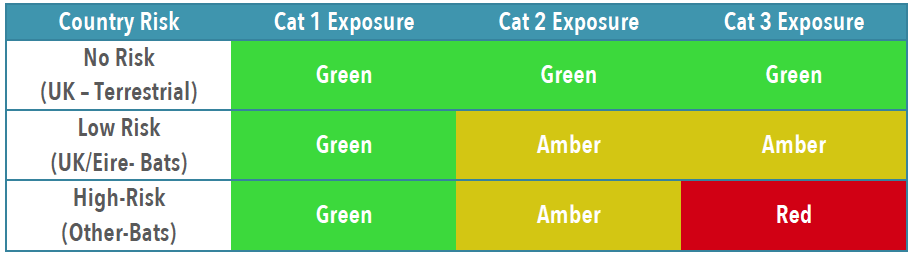
In the UK the only bat to carry rabies is the Daubenton’s Bat [Picture on the Left] and this is not a common bat in the UK. The UK and Ireland are Classified as “low-risk” for bat exposure. Despite our “low-risk” status in 2002 a man died from rabies caught in the UK from bat exposure.
Although rabies is rare it is fatal so we must treat appropriately, Public Health England – Green book details this.
To establish patients risk and thus treatment you need to establish the Exposure Category and Country Risk [Link to Country Risk]

Obviously patients with wounds will need appropriate wound care and cleaning, specifics for rabies are below.
If in ANY doubt, or you feel you need advice about treatment contact: On-Call Microbiologist (who will contact PHE or Virology advice)

You will likely need to liaise with the duty pharmacist to obtain vaccine or HRIG – which may need to be sent from a different hospital. [it is probably worth trying to obtain the 1st weeks treatment if possible, to avoid treatment delays]
IN HOURS 08:30AM-5PM PLEASE CALL PHARMACY TO INFORM THEM TO EXPECT A DELIVERY OF IMMUNOGLOBULIN SO THIS CAN BE SEGREGATED FOR THE CORRECT PATIENT. PLEASE ASK TO SPEAK TO THE RESPONSIBLE PHARMACIST CRH (4218/4279) HRI (2422/7123)
Rabies and Immunoglobulin Service (RIgS), National Infection Service, Public Health England, Colindale (PHE Colindale Duty Doctor out of hours): 0208 327 6204 or 0208 200 4400
This is guide to the investigation of Metastatic Spinal Cord Compression (MSCC) in Oncology/Haematology patients. – (Trust link)
You need to be a bit more suspicious and have a lower threshold for investigation than in patients without Known, Suspected OR Previous Malignancy Read more
Unfortunately under 1 year olds are at a higher risk of NAI and this needs to be considered in ALL presentations. But remember if the child can’t Crawl/Stand/Cruise/Walk they shouldn’t injure themselves.
 the iNFANT is truly a design enigma, it is simple yet complicated, amazing yet frustrating, beautiful yet disgusting. And due to a unique production method, each iNFANT has its own variations and special features. Read more
the iNFANT is truly a design enigma, it is simple yet complicated, amazing yet frustrating, beautiful yet disgusting. And due to a unique production method, each iNFANT has its own variations and special features. Read more
In our trust we don’t have paediatric critical care beds. However, in our region we use EMBRACE (a paediatric critical care transport team), who can transfer critically ill children to specialist centers (in or out of region).
This is a relatively common presentation within the ED that has a myriad of possible diagnoses ranging from sprain to malignancy. One thing to remember is that patients and relatives will look for a traumatic reason for limb pain, and may link it to minor injuries that would not have caused it. Read more
To maintain or restore patency of the ductus arteriosus
Only to be used in infants who are ventilated or where ventilation is immediately available
DO NOT DELAY IN STARTING Alprostadil if: there is clinical
suspicion of duct dependent CHD while waiting for paediatric cardiology opinion OR echocardiogram, even when in-house echo facilities are present.
PDF: Alprostidil
Paediatric Hypoglycaemia (BM <2.6) is a relatively common presentation in the Emergency Department. However, if we don’t do the BM it’s easy to miss.
Hypoglycaemia in paediatric diabetic patients is managed separately – see here
Hypoglycaemia in neonates (<72 hours of life) also has specific management – see here (Flowcharts A + B)
Hypoglycaemia is generally caused by disruption in one of the following:
Diabetic Ketoacidosis – remember in paediatrics this may be the 1st presentation of diabetes.
DKA Management Flow Chart – HERE