High Consequence Infectious Diseases (HCIDs) include a group of rare but severe infections that require
ACTIONS – CARD HERE
- Immediate isolation
- Enhanced PPE
- Early specialist involvement.
High Consequence Infectious Diseases (HCIDs) include a group of rare but severe infections that require

Severe pain is the most common reason that patients with sickle cell, will attend the ED. The pain can be agonising (and often underestimated by us), we need to act fast to help ease the symptoms
Read more
In the case of patient with Massive Haemorrhage weather that be from Trauma, Surgical, O&G, UGIB, you can activate the MHP

Aortic Dissection (AD), is uncommon (1 AD:200 ACS) but is…Rapidly FATAL! Unfortunately recognising aortic dissection is difficult with a clinician pickup rate of 15-43%. Read more
Penthrox is an inhaled, patient controlled analgesic for use with moderate to severe acute pain associated with trauma. Not to be used in atraumatic pain, chronic pain, children or pregnancy.
Rapid onset of analgesia lasting 25-60 minutes depending on rate and depth of inhalation. Wears off 10 minutes after last inhalation.
Recent Incident: Bat contact was not recognised (effectively touching a bat without gloves means treatment is recommended)
Important: Rabies Vaccine is in short supply and we must do a UKHSA risk assessment. Call RIgS 09:30-17:00 7 days, OR complete Form

Rabies is an acute viral encephalomyelitis caused by members of the lyssavirus genus. The UK has been declared “Rabies-Free”. However, it is known that even in “Rabies-Free” counties the bat population posse a risk.
In the UK the only bat to carry rabies is the Daubenton’s Bat [Picture on the Left] and this is not a common bat in the UK. The UK and Ireland are Classified as “low-risk” for bat exposure. Despite our “low-risk” status in 2002 a man died from rabies caught in the UK from bat exposure.
Although rabies is rare it is fatal so we must treat appropriately, Public Health England – Green book details this.
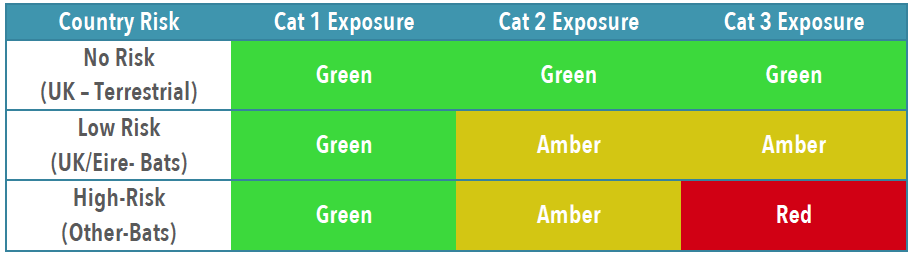
To establish patients risk and thus treatment you need to establish the Exposure Category and Country Risk [Link to Country Risk]

Obviously patients with wounds will need appropriate wound care and cleaning, specifics for rabies are below.
If in ANY doubt, or you feel you need advice about treatment contact: On-Call Microbiologist (who will contact PHE or Virology advice)

You will likely need to liaise with the duty pharmacist to obtain vaccine or HRIG – which may need to be sent from a different hospital. [it is probably worth trying to obtain the 1st weeks treatment if possible, to avoid treatment delays]
IN HOURS 08:30AM-5PM PLEASE CALL PHARMACY TO INFORM THEM TO EXPECT A DELIVERY OF IMMUNOGLOBULIN SO THIS CAN BE SEGREGATED FOR THE CORRECT PATIENT. PLEASE ASK TO SPEAK TO THE RESPONSIBLE PHARMACIST CRH (4218/4279) HRI (2422/7123)
Rabies and Immunoglobulin Service (RIgS), National Infection Service, Public Health England, Colindale (PHE Colindale Duty Doctor out of hours): 0208 327 6204 or 0208 200 4400
Fitting ASPEN collars is import – for both the comfort and function of the collar. The DENS study has been looking at the effectiveness on collars in peg fractures. Preliminary results suggest limited benefit, which made be due to the fact the many patients remove the collar early as not comfortable.
MEOWS is the early warning score used during Pregnancy and 6 weeks postpartum.

Although in ED we cannot prevent the primary injury, our objective is to recognise and prevent secondary injury. Through the use of the agreed standards
| Option | Scenario | Action | |
| 1 | This investigation demonstrates an injury that may affect spinal stability. (see Notes) | Continue spinal protection and seek advice from an appropriate clinical team. | |
| 2 | This scan is of good quality and there are no comorbidities confounding its interpretation. No features of instability, such as fracture, haematoma or joint disruption are seen. | Patients with NO acute neurological symptoms/signs on examination or mobilisation. | Spinal protection may be removed. |
| Patient who HAS acute neurological symptoms/signs on examination or mobilisation. | Continue spinal protection and seek advice from an appropriate clinical team. | ||
| Unconscious OR unable to Co-Operate with examination (see Notes) | Spinal protection can be removed with caution providingConsultant Radiology report & No evidence of acute neurological deficitIt must be recognised there is a <1% chance of unrecognised injury. ANY evidence of neurological deterioration should be re-immobilised pending MRI | ||
| 3 | Whilst there are no obvious features of spinal instability, the CT scan is either not of good quality and/or there are comorbidities confounding its interpretation. | Continue spinal protection until MRI is performed and report available. | |
This pragmatic approach is in line with BOA-Standards, however, it must be recognised there is a chance of deterioration. If ANY evidence of neurological deficit the patient should be re-immobilised and reassessed for further imaging.